What is pyloric stenosis?
Pylorus is the name of the muscle between the stomach and the small intestine. Stenosis means that an opening is smaller than it should be.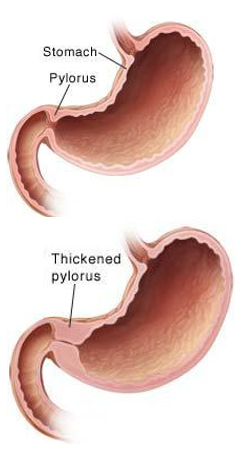
Pyloric stenosis means that the muscle between the stomach and the intestine is too thick. The thick muscle stops food from going into the intestine as it should.
Pyloric stenosis almost always happens in the first few months of life. Most patients are around 4 to 6 weeks old.
What are the symptoms?
Pyloric stenosis makes your baby throw up (vomit). At first, your baby may only throw up once in a while. As time goes by, your baby will throw up more often and in larger amounts. With time, all feedings may be thrown up. The vomit may be forceful enough to shoot across the room. This is called projectile vomiting. If your baby throws up a lot, it can cause:
- Dehydration. This means a loss of too much fluid.
- Unbalanced electrolytes. Electrolytes are the salt levels in the blood stream.
- Poor nutrition and weight loss.
- With treatment, pyloric stenosis does not cause any long-term problems. Your baby will be able to eat and digest food again.
What tests may be done?
- Physical exam. The doctor will check your baby and try to feel for a lump in their belly. This lump is the thickened pyloric muscle. It feels like an olive. You may hear the doctors talk about the olive.
- Ultrasound. This ultrasound is like the ones used during pregnancy. A special wand and gel on the outside of your baby’s belly is used. It will show if there is a thickening around the pyloric muscle. It will not hurt. An Ultra Sound is the best test for diagnosing pyloric stenosis.
- Blood test. This will check to see if your baby is dehydrated.
- UGI. This is an x-ray. UGI means upper gastro-intestinal. This x-ray helps the doctor see if your baby has pyloric stenosis. It is only necessary if the ultrasound is doesn’t tell us what we need to know. Ask for the UGI handout. It will help you understand more about this test.
How is it treated?
- Surgery called pyloromyotomy is needed. The surgery takes about one hour.
Most pediatric surgeons now do this surgery using small incisions (cuts less than 5mm) and a camera called a laparoscope. The thickened muscle is cut, but not taken out. This will let food move freely into the intestine. Your baby will have one or more incisions depending on how the surgery was done. The doctor will tell you what to expect. Using a laparoscope makes the scars mostly invisible once healed.
How will my baby be prepared for surgery?
- If your baby is dehydrated or has unbalanced electrolytes, an IV will be used to give your baby fluids.
- If your baby had a UGI, the barium swallowed during the x-ray will be removed.
- A small tube is put in your baby's nose or mouth. The tube, called an NG tube, is passed into the stomach.
- A salt-water solution will go through the tube and into the stomach. The solution mixes with the barium to thin it. This will help it come out easier.
- After the barium and salt water is removed, the tube is taken out. In some cases the tube is left in for surgery.
- Surgery will be done be about 12 to 24 hours later, when your baby is no longer dehydrated and their electrolytes are normal.
- We may use machines to watch your baby’s heart rate and breathing. They will be used for 12 hours after surgery.
- If your baby still has an umbilical cord stump it will be cleaned with a special solution.
What happens after surgery?
- The doctor will cover the incision with Steri-Strips® or a glue that holds the incision together. If Steri-Strips are used, there might be a small gauze or clear bandage over them. This cover will be removed the day after the surgery.
- After surgery your baby will go to the recovery room. The nurses and doctors will closely watch your baby. After waking up, your baby will go back to their room.
-
The pain from the surgery is often well managed, using:
- numbing medicine placed during the surgery,
- Tylenol after surgery, and
- you holding your baby to provide comfort.
- The IV will stay in until your baby is eating well.
- Feedings are normally started 3 hours after surgery. Your baby will be fed breast milk from a bottle or formula if they are hungry. Your baby should not have more than 60 ml’s for the 5 feedings.
- They may eat as often as needed but should not wait longer than 4 hours. You may leave after your baby has had 5 feedings without throwing up. The last 2 must be at least 30 ml’s.
- Your baby may spit-up or vomit a little bit after surgery. This is normal. Most often this stops within a few days. Your baby should eat slowly and burp often to prevent vomiting.
- Most babies go home within 24 hours after the surgery.
What will I need to do at home?
- Keep the incision dry. Only give sponge baths for the first 3 days. Keep soap, powder and ointments away from the incision.
- Remove the Steri-Strips ten days after the surgery.
- Check the incision every day. Look for signs of infection. Signs include redness, swelling, drainage or fever.
- Babies who recover from pyloric stenosis do not require a special diet and rarely have long-term problems from the surgery or pyloric stenosis.
Draft Number: 1066Revision: October 21, 2025