Provided by "Pediatric Heart Surgery — a reference for professionals"
Patient families can visit our ventricular septal defect page for more information and answers to common questions.
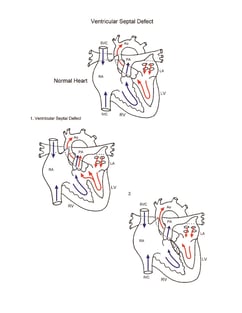
Pathophysiology
Surgical technique
Repair of ventricular septal defect requires cardiopulmonary bypass and aortic cross clamping. Most ventricular septal defects are repaired via right atriotomy and are visualized through the tricuspid valve. A patch of autologous pericardium or synthetic material is used to close the defect. Care is taken to avoid atrioventricular conduction tissue, as this can result in loss of normal atrioventricular conduction postoperatively. Transesophageal echocardiography is used to help assess adequacy of repair. Comparison of mixed venous and pulmonary arterial oxygen saturation is performed to rule out residual ventricular septal defect. Cardiopulmonary bypass time and aortic cross-clamp time required for repair of ventricular septal defects are usually short to moderate.
Postoperative considerations
The postoperative course following isolated VSD closure is usually uncomplicated. Invasive monitors used include arterial, central venous, and left atrial catheters. A pulmonary artery pressure monitoring catheter is sometimes used when preoperative pulmonary artery hypertension exists. Non-invasive monitors might include NIRS (near-infrared spectroscopy) probes to assess adequacy of regional and global perfusion and traditional pulse oximetry. Vasoactive infusions required for hemodynamic management might include epinephrine, milrinone, and/or nitroprusside. When surgical intervention is delayed in patients with non-restrictive VSD, long- standing pulmonary artery hypertension can result in a more complex postoperative course. Sedation with infusions of fentanyl and a neuromuscular blocking agent is instituted to manage pulmonary artery hypertension. Inhaled nitric oxide has proven useful in reducing pulmonary vascular resistance and pressure. Atrioventricular conduction abnormalities are occasionally encountered following repair of ventricular septal defects. Edema around the VSD sutures can cause acute development of transient heart block, requiring temporary pacing. Atrioventricular pacing capability should be readily available. Excessive postoperative bleeding is rare. Length of hospital stay required following repair averages 5 to 7 days.