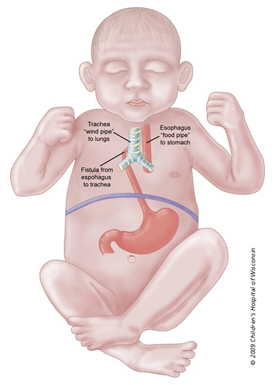
Tracheal Esophageal Fistula and Esophageal Atresia (TEF/EA) is when blind pouch of the esophagus with a fistula from the lower esophageal segment connects with the trachea. This is the most common type and accounts for 86% of cases.
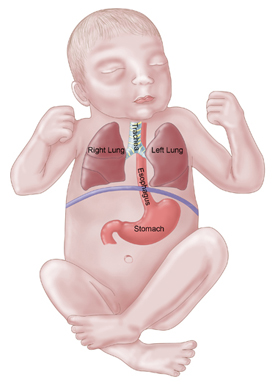
The trachea is the windpipe and goes to the lungs. The esophagus is the "food pipe" and goes to the stomach. They run side-by-side through the neck and upper chest. Normally the trachea and the esophagus are not connected in any way. Very early in the development of a fetus a single tube will divide to form the esophagus and the trachea. For an unknown reason, sometimes the wall does not form properly and a tracheal esophageal fistula and/or esophageal atresia may be the result.
A fistula is an abnormal connection and atresia means a blockage. An esophageal atresia is a blockage in the esophagus, which can occur with or without a fistula. There are a variety of ways the esophagus and trachea can be connected with a fistula.
The five most common variations of a TEF are:
- A middle section of the esophagus is missing and the windpipe is connected to the lower end of the esophagus with a fistula. This is the most common type and accounts for 86% of cases.
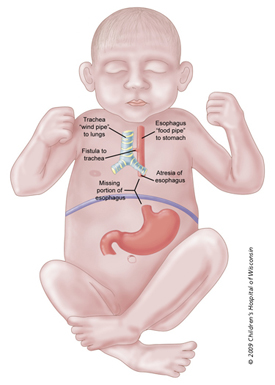
- An absence of a portion of the esophagus with no fistula to the trachea where neither end is connected to the windpipe. This is more rare accounting for 8% and is a true esophageal atresia (with no fistula).
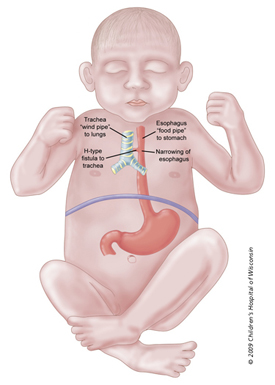
- The esophagus is complete (but may have a portion that is too narrow) with a fistula to the trachea. This is an H-type and accounts for 4% of cases.
- A middle section of the esophagus is missing and there is a fistula to the trachea from the upper portion of the esophagus. This accounts for 1% of cases.
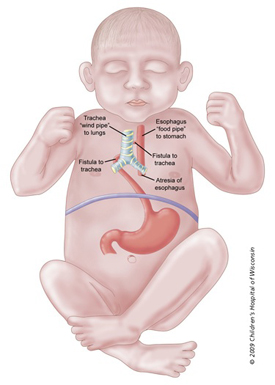
- An absence of a portion of the esophagus with fistula connections to the trachea from both the upper and lower portions of the esophagus. This accounts for 1% of cases.
TEF/EA is one of the most common gastrointestinal birth defects. It has a slightly higher incidence in males than females. The incidence rate of TEF/EA is approximately one in 4,000 live births. Of the babies born with TEF/EA, approximately 50% will have an associated birth defect. The most commonly associated birth defect is cardiac, seen in about 25% of these patients. Atrial and ventricular septal defects are the most common cardiac disorders seen. We do not know the cause of TEF/EA but it is thought to occur around the fourth week of pregnancy as the various systems are developing. We know it is not due to anything the mother did or did not do during pregnancy.
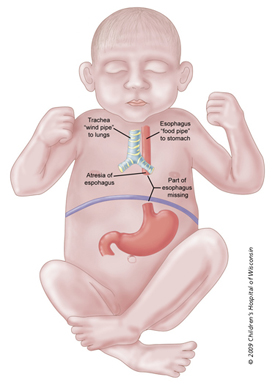
An absence of a portion of the esophagus with no fistula to the trachea. Each end is a blind pouch. This is more rare, accounting for 8% of cases, and is a true esophageal atresia with no fistula.
Occasionally there will be a clustering of birth defects along with the TEF/EA, but no genetic association has been found. The acronym VACTERL is used to describe this combination of birth defects. Each letter of the acronym stands for a type of anomaly:
- Vertebral anomalies
- Anus, imperforate
- Cardiac
- Tracheo-Esophageal fistula or atresia
- Renal anomalies
- Limb anomalies (radial dysplasia)