
In this section
Twin-twin transfusion syndrome (TTTS)
What is twin-twin transfusion syndrome?
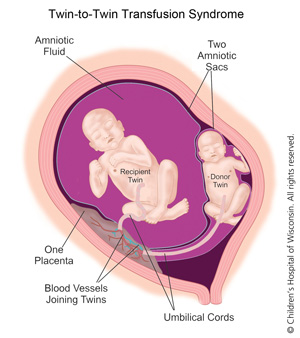
Twin-twin transfusion syndrome is an imbalance in the blood flow between identical twins who share one placenta known as monochorionic twins but have separate amniotic sacs. Twins who share a placenta but have separate amniotic sacs are known as monochorionic-diamniotic twins.
When the placenta is shared, blood vessels within it connect the twins' blood supply, allowing blood to flow between them. If the blood flow becomes unequal, the twins will grow at different rates with the smaller (donor) twin pumping blood to the larger (recipient) twin. The condition is found in about 15 percent of monochorionic-diamniotic twin pregnancies.
Prenatal Diagnosis of TTTS
A prenatal ultrasound will show if identical twins are present, if the placenta is shared and if two amniotic sacs are in place. This confirms a monochorionic-diamniotic twin pregnancy with increased risk of TTTS. In these cases, your obstetrician will most likely refer you to a maternal-fetal medicine specialist also known as perinatologist, who specializes in high-risk pregnancies.
Ultrasounds will be repeated frequently to monitor for signs of TTTS, including an enlarged uterus, fetuses of differing sizes and varying amniotic fluid levels in the amniotic sac. A fetal echocardiogram may be ordered to screen for heart failure if one twin is larger than the other.
How does TTTS affect my babies?
As a result of their differing blood supplies, each twin faces a set of challenges that require expert and experienced care. The donor twin gets less blood than its sibling, causing it to become anemic (lacking in red blood cells) and produce less urine, the main ingredient of amniotic fluid. The fluid can continue to decrease (oligohydramnios) to the point of disappearing completely, causing the amniotic sac to cling to the fetus. The fetus may also appear to adhere to the wall of the womb, prompting many to refer to this twin as the "stuck twin."
The recipient twin, meanwhile, will struggle with opposite concerns. Too much blood will lead to excess urine production, potentially resulting in a large bladder and hydrops, a prenatal form of heart failure. Excess urine will increase the amniotic fluid (polyhydramnios) around the recipient twin and cause the womb to over-expand. If TTTS is untreated, premature labor and delivery often results, with the possible loss of one or both babies.
If just one of the twins survives, that twin is at risk for brain and other organ damage due to inadequate oxygen and blood flow. This can occur because the shared blood circulation increases the chance of the blood flowing in the opposite direction. Pumping blood back to the deceased twin deprives the surviving twin of oxygen, fluids and nutrients. The surviving twin may also be at risk for restricted growth and other complications while in the womb.
Most TTTS twins, whether they receive treatment or not, will be born prematurely.
How does TTTS affect the pregnancy?
Mothers pregnant with monochorionic-diamniotic twins may experience rapid uterine growth, premature contractions and shortness of breath, all signs of excess amniotic fluid. These conditions often start to occur about 20 weeks into pregnancy. If you experience these symptoms, immediately contact your physician.
If the twins' conditions do not require immediate attention, mothers will be closely monitored by ultrasound and fetal echocardiograms throughout pregnancy. Physicians will watch for signs that the cervix is weakening, which increases the risk for premature delivery. They also will monitor the twins for heart failure, soft tissue swelling, abnormal and/or differing fluid volumes and abnormal blood flow in the umbilical arteries. These are all indications that the condition of the fetuses is deteriorating and that additional intervention may be needed.
When excess amniotic fluid is a concern, bed rest or reclining in a horizontal position will be recommended. This will help reduce pressure on the cervix and improve blood flow to the uterus and kidneys. Some research suggests that mothers with pregnancies complicated by TTTS may have lower protein levels in their blood than other pregnant women. It may be recommended that mothers with TTTS pregnancies consider additional protein through nutrition supplements such as protein shakes.
Delivery: This occurs if the pregnancy is beyond 25 weeks and the twins are believed to be healthy enough to survive. If delivery is not an option and treatment is needed prior to delivery, there are three potential approaches.
Amnioreduction: This method is used later in pregnancy or if complications rule out laser ablation treatment. Amnioreduction allows physicians to drain away some of the excess amniotic fluid surrounding the larger twin. This will make the mother more comfortable, reduce the chance of premature labor and better equalize the flow of blood between the fetuses. Amnioreduction is an outpatient procedure and no hospital stay is required unless there are other circumstances that make it necessary. The procedure may need to be repeated through the course of the pregnancy.
Fetoscopic laser ablation (minimally invasive): Fetoscopic laser ablation of the shared placental vessels is a state-of-the-art and increasingly successful treatment aimed at disconnecting the shared blood vessels between the twins in the placenta. This stops the unhealthy blood transfer between them. Fetoscopic laser ablation is only offered by specially trained physicians at select treatment centers like the Fetal Concerns Center. It is most often conducted between 16 to 26 weeks of pregnancy. Studies show an 80 to 85 percent survival rate for at least one twin following laser ablation and an overall twin survival rate of 65 to 70 percent. In fact, at Children's Wisconsin, we have a 93% survival rate of at least one baby and 80% survival rate of both babies after laser ablation procedures.* The approach also greatly reduces the risk of neurological damage to the babies before birth.
During laser ablation, a physician inserts a tiny scope (fetoscope) through the uterus to find the blood vessels connecting the twins. The laser seals off the shared vessels so that each fetus now will have his or her own circulation.
Cord Coagulation: In the most severe cases where there is no chance for the donor twin to survive, a procedure called cord coagulation may be performed. The surgeon will completely close off the blood supply to a failing donor twin so that the recipient twin may thrive. This is considered a last option.
*Based on data from 2012 - 2016.
What about after laser ablation or surgery?
After laser ablation or any prenatal treatment, mothers are typically admitted to the hospital for two to three days for monitoring. They are then discharged for ongoing care by their obstetrician. Bed rest will likely be recommended and medications prescribed to prevent premature delivery.
Patients may require additional ultrasounds for continued monitoring throughout the pregnancy.
Will I be able to help care for my babies?
Yes, ask your nurse about ways to interact with and care for your babies. Babies that are healthy at birth may need only a brief stay in a special care nursery. Others may need more time in the NICU to resolve health issues.
Many mothers are able to successfully breast feed their twins. Lactation specialists can help mothers of multiples learn techniques for breastfeeding their babies separately and together, and to increase their milk supply. Mothers whose babies are unable to breastfeed because they are sick or premature can pump their breast milk and store the milk for later feedings.
Families with more than one baby need help from family and friends, especially if the pregnancy was complicated and there are other siblings at home. Having help will allow mothers more time to get to know their babies, take care of feedings and rest and recover from delivery.
When can my babies go home?
How long your babies remain hospitalized will vary depending on their conditions. Once babies are able to feed, grow and stay warm, they can usually be discharged.
What's is the long-term prognosis for my babies?
The majority of TTTS twins who have appropriate treatment during pregnancy will survive and the majority of survivors will be normal and healthy. If untreated, the survival rate for TTTS twins is approximately 10 to 15 percent.
Once TTTS babies are born, blood supply sharing is no longer a factor. They may face concerns resulting from prematurity or the effects of TTTS inside the womb. Low birth weight babies have an increased risk of long-term neurological problems such as mental retardation, cerebral palsy, vision loss and hearing loss. Babies born between 24 and 32 weeks have a higher risk of handicaps.
What about future pregnancies?
The chance of TTTS occurring in future pregnancies is the same as in the first (approximately 1 in 1,000 pregnancies) and does not increase following a TTTS pregnancy.
What other additional resources are available?
The Twin-Twin Transfusion Syndrome Foundation
www.tttsfoundation.org
Fetal surgery for TTTS leads to healthy delivery
A Milwaukee Magazine article discusses the care a mother received for twin-twin transfusion syndrome during her pregnancy.
{kind=link}
Contact us
For additional information on the Fetal Concerns Center at Children's Wisconsin, please call:
(414) 337-4776
Fax: (414) 337-1884
Note: These phone numbers should not be used for urgent medical concerns. Please contact your physician directly if your situation requires immediate attention, or dial 911 if it is an emergency.