
In this section
Hypoplastic left heart syndrome (HLHS)
Interstage home monitoring | What is HLHS? | Causes | Symptoms | Diagnosis | Treatment | Postoperative care | Home care | Long-term outlook
Hypoplastic left heart syndrome (HLHS) is an uncommon, complex congenital (present at birth) defect in which several structures in the heart’s left side form incorrectly. It is one of several “single ventricle defect” conditions where only one of the heart’s two ventricles can pump effectively. Babies with HLHS cannot properly pump oxygen-rich blood to the body, and therefore cannot live without intervention.
Worldwide leaders in Hypoplastic left heart syndrome (HLHS) surgery survival rates
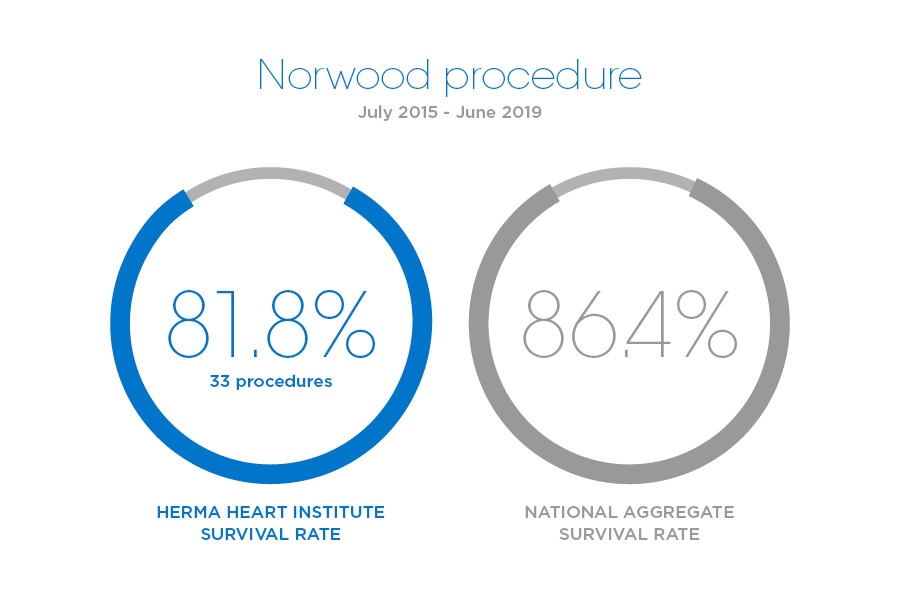
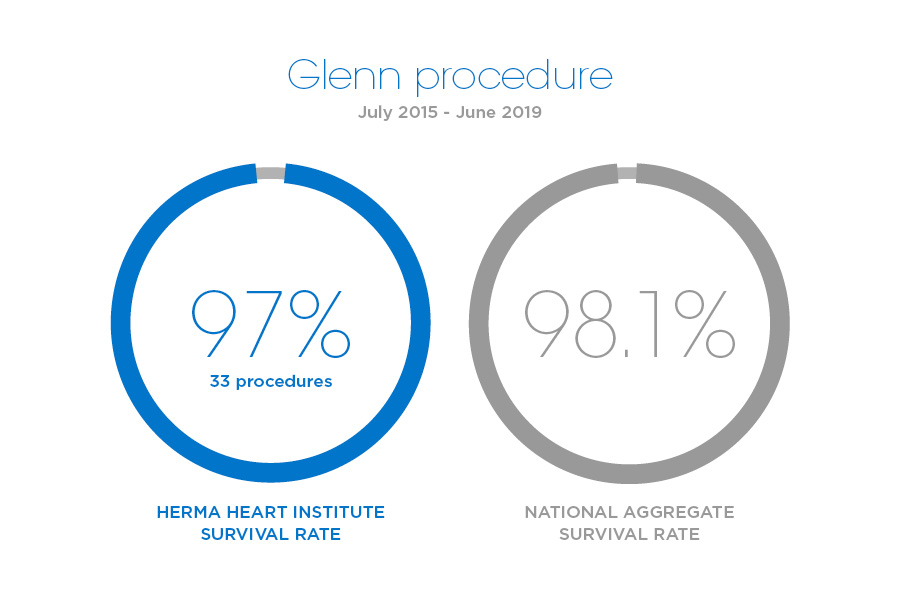
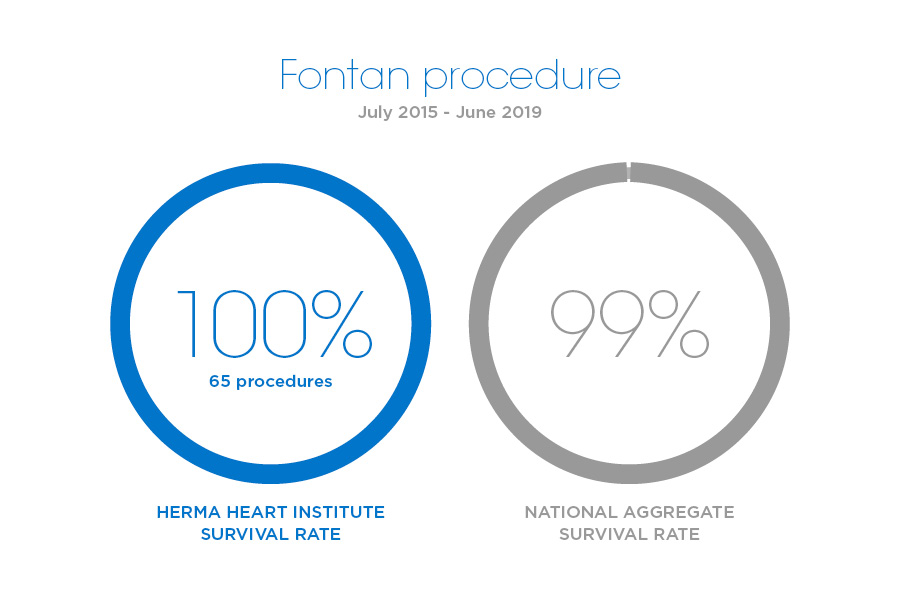
Herma Heart Institute specializes in repairing Hypoplastic left heart syndrome and single ventricle defects, and has the best published HLHS survival rates worldwide. Our institute consistently outperforms when it comes to congenital heart surgery outcomes for even the most complex types of heart disease, as evaluated by the Society of Thoracic Surgeons. Treatment for HLHS requires our highly specialized congenital heart surgeons to rework the baby's circulatory system through a series of three open heart surgeries (Norwood, Glenn, and Fontan procedures) staged over a span of about three years. An alternative approach is heart transplantation, also an area of expertise at Children's Wisconsin. See survival rate outcomes specific to the Norwood, Glenn and Fontan procedures.
Interstage home monitoring
For children undergoing Hypoplastic Left Heart Syndrome surgical treatment, the time between the first and second procedures, commonly known as the “interstage period,” is a critical stage in their care. Research has proven that careful monitoring of the child’s condition can prevent serious complications, ensure optimal growth and improve both survival and quality of life.
The Herma Heart Institute at Children's Wisconsin in Milwaukee is recognized for pioneering the first interstage home monitoring initiative of its kind for partnering with parents in caring for infants with HLHS and other single ventricle defects. The experience of Children’s Interstage Home Monitoring Program has helped significantly boost survival rates among babies with HLHS and is now the standard of care worldwide.
What is hypoplastic left heart syndrome?
Hypoplastic left heart syndrome (HLHS) is a combination of several abnormalities of the heart and great blood vessels. It is a congenital syndrome, meaning that the heart defects occur due to abnormal underdevelopment of sections of the fetal heart during the first 8 weeks of pregnancy.
In the normal heart, oxygen-poor (blue) blood returns to the right atrium from the body, travels to the right ventricle, then is pumped through the pulmonary artery into the lungs where it receives oxygen. Oxygen-rich (red) blood returns to the left atrium from the lungs, passes into the left ventricle, and then is pumped out to the body through the aorta.
In hypoplastic left heart syndrome, also known as single ventricle defect, most of the structures on the left side of the heart are small and underdeveloped. The degree of underdevelopment differs from child to child. The structures affected usually include the following:
- Mitral valve - the valve that controls blood flow between the left atrium and left ventricle in the heart.
- Left ventricle - the lower left-hand chamber of the heart. It receives oxygen-rich (red) blood from the left atrium and pumps it into the aorta, which takes the blood to the body. The left ventricle must be strong and muscular in order to pump enough blood to the body to meet its requirements.
- Aortic valve - the valve that regulates blood flow from the heart into the aorta.
- Aorta - the largest artery in the body and the primary blood vessel leading from the heart to the body.
Perhaps the most critical defect in HLHS is the small, underdeveloped left ventricle. This chamber is normally very strong and muscular so it can pump blood to the body. When the chamber is small and poorly developed, it will not function effectively and cannot provide enough blood flow to meet the body's needs. For this reason, an infant with hypoplastic left heart syndrome will not live long without surgical intervention.
- Hypoplastic left heart syndrome occurs in up to four out of every 10,000 live births.
- The syndrome comprises 8 percent of all cases of congenital heart disease.
- It is one of the top three heart abnormalities to cause problems in the newborn.
- HLHS occurs slightly more often in boys than in girls.
Hypoplastic left heart syndrome causes and risk factors?
Some congenital heart defects may have a genetic link, either occurring due to a defect in a gene, a chromosome abnormality, or environmental exposure, causing heart problems to occur more often in certain families. In hypoplastic left heart syndrome, there may be abnormalities of other organs, such as diaphragmatic hernia, omphalocele, and hypospadias.
In many children, HLHS occurs sporadically (by chance), with no clear reason evident for their development.
What are the symptoms of hypoplastic left heart syndrome?
Infants and babies with HLHS usually develop symptoms shortly after birth. The following are the most common symptoms of hypoplastic left heart syndrome. However, each child may experience symptoms differently. HLHS symptoms may include:
- Cyanosis (blue color of the skin, lips, and nailbeds)
- Pale skin
- Sweaty or clammy skin
- Cool skin
- Heavy and/or rapid breathing
- Fast heart rate
The symptoms of hypoplastic left heart syndrome may resemble other medical conditions and heart problems. Always consult your child's physician for a diagnosis.
How is hypoplastic left heart syndrome diagnosed?
Your child's physician may have heard a heart murmur during a physical examination, and referred your child to a pediatric cardiologist for a diagnosis. A heart murmur is simply a noise caused by the turbulence of blood flowing through the obstruction from the right ventricle to the pulmonary artery. Symptoms your child exhibits will also help with the diagnosis.
A pediatric cardiologist specializes in the diagnosis and medical management of congenital heart defects, as well as heart problems that may develop later in childhood. The cardiologist will perform a physical examination, listening to the heart and lungs, and make other observations that help in the diagnosis. However, other tests are needed to help with the diagnosis.
Chest X-ray - a diagnostic test which uses invisible electromagnetic energy beams to produce images of internal tissues, bones, and organs onto film.
Electrocardiogram (ECG or EKG) - a test that records the electrical activity of the heart, shows abnormal rhythms (arrhythmias or dysrhythmias), and detects heart muscle damage.
Echocardiogram (echo) - a procedure that evaluates the structure and function of the heart by using sound waves recorded on an electronic sensor that produce a moving picture of the heart and heart valves.
Hypoplastic left heart syndrome - Treatment
Specific hypoplastic left heart syndrome treatment will be determined by your child's physician based on:
- Your child's age, overall health, and medical history
- Extent of the disease
- Your child's tolerance for specific medications, procedures, or therapies
- Expectations for the course of the disease
- Your opinion or preference
Your child will most likely be admitted to the intensive care unit (ICU) or special care nursery once symptoms are noted. Initially, your child may be placed on oxygen, and possibly even on a ventilator, to assist his/her breathing. Intravenous (IV) medications may be given to help the heart and lungs function more efficiently.
There are two approaches offered to treat HLHS. Your child's cardiologist and cardiac surgeon will explain the risks and benefits to you. The options include the following:
- A series of three operations done in stages to establish the heart's right ventricle as the main pumping chamber and to reroute blood flow through several surgically created connections. The three operations include:
- The Norwood procedure, done shortly after birth
- The Glenn procedure, performed at about six months
- The Fontan procedure, performed at about 18 months
- Heart transplantation
HLHS postoperative care for your child
After each surgery, infants will return to the cardiac intensive care unit (CICU) to be closely monitored during recovery.
- Ventilator - a machine that helps your child breathe while he/she is under anesthesia during the operation. A small, plastic tube is guided into the windpipe and attached to the ventilator, which breathes for your child while he/she is too sleepy to breathe effectively on his/her own. After a HLHS operation, children will benefit from remaining on the ventilator overnight or even longer so they can rest.
- Intravenous (IV) catheters - small, plastic tubes inserted through the skin into blood vessels to provide IV fluids and important medicines that help your child recover from the operation.
- Arterial line - a specialized IV placed in the wrist or other area of the body where a pulse can be felt, that measures blood pressure continuously during surgery and while your child is in the CICU.
- Nasogastric (NG) tube - a small, flexible tube that keeps the stomach drained of acid and gas bubbles that may build up during surgery.
- Urinary catheter - a small, flexible tube that allows urine to drain out of the bladder and accurately measures how much urine the body makes, which helps determine how well the heart is functioning. After surgery, the heart will be a little weaker than it was before, and, therefore, the body may start to hold onto fluid, causing swelling and puffiness. Diuretics may be given to help the kidneys to remove excess fluid from the body.
- Chest tube - a drainage tube may be inserted to keep the chest free of blood that would otherwise accumulate after the incision is closed. Bleeding may occur for several hours, or even a few days after surgery.
- Heart monitor - a machine that constantly displays a picture of your child's heart rhythm, and monitors heart rate, arterial blood pressure, and other values.
Your child may need other equipment not mentioned here to provide support while in the CICU, or afterwards. The hospital staff will explain all of the necessary equipment to you.
Your child will be kept as comfortable as possible with several different medications; some which relieve pain, and some which relieve anxiety. The staff will also be asking for your input as to how best to soothe and comfort your child.
After being discharged from the CICU, your child will recuperate in another hospital unit before going home. You will learn how to care for your child at home before your child is discharged. Your child may need to take medications for a while, and these will be explained to you. The staff will give you instructions regarding medications, activity limitations, and follow-up appointments before your child is discharged.
Infants who spent a lot of time on a ventilator, or who were fairly ill while in the CICU, may have trouble feeding initially. These babies may have an oral aversion; they might equate something placed in the mouth, such as a pacifier or bottle, with a less pleasant sensation such as being on the ventilator. Some infants just are tired, and need to build their strength up before they will be able to learn to bottle-feed. Strategies used to help infants with nutrition include the following:
- High-calorie formula or breast milk - Special nutritional supplements may be added to formula or pumped breast milk that increase the number of calories in each ounce, thereby allowing your baby to drink less and still consume enough calories to grow.
- Supplemental tube feedings - Feedings given through a small, flexible tube that passes through the nose, down the esophagus, and into the stomach, that can either supplement or take the place of bottle-feedings. Infants who can drink part of their bottle, but not all, may be fed the remainder through the feeding tube. Infants who are too tired to bottle-feed at all may receive their formula or breast milk through the feeding tube alone. Learn more about our Enteral Feeding Program.
Caring for your child at home following a HLHS surgery
Pain medications, such as acetaminophen or ibuprofen, may be recommended to keep your child comfortable at home. Your child's physician will discuss pain control before your child is discharged from the hospital.
If any special treatments are to be given at home, the nursing staff will ensure that you are able to provide them, or a home health agency may assist you.
You may receive additional instructions from your child's physicians and the hospital staff. Families will also be referred to our Neurodevelopmental Follow-up Program, where our specialists will monitor and encourage your child's healthy development for living life to the fullest.
Long-term prognosis for hypoplastic left heart syndrome
Consult your child's physician regarding the specific HLHS prognosis for your child. For outcomes relating to the series of surgeries to correct hypoplastic left heart syndrome, see the information about the Norwood, Glenn and Fontan procedures.
Let us help you
Coming from out of town?
Traveling with a sick child to a new city can be stressful. We can make your visit to our hospital as easy as possible.
Traveling here locally?
Contact us for more information about the Herma Heart Institute. Request an appointment online or call (414) 607-5280 or toll-free (877) 607-5280.